Impact on NHS workforce and resources
This NICE guideline on renal and ureteric stones: assessment and management has been reviewed for its potential impact on the NHS workforce and resources. The guideline offers best practice advice on the assessment and management of renal and ureteric stones.
Recommendations likely to have an impact on resources
The recommendations that are most likely to have a substantial resource impact are:
- Recommendation 1.5.3 For adults (16 years and over) offer shockwave lithotripsy (SWL) to treat ureteric stones less than 10 mm. Consider ureteroscopy if a previous course of shockwave lithotripsy has failed.
- Recommendation 1.5.5 Consider alpha blockers as adjunctive therapy for adults having SWL for ureteric stones less than 10 mm.
Context
Around 22,000 people in England had treatment for ureteric stones in 2016/17 (NHS Digital, Hospital Episodes Statistics).
Treatment for renal and ureteric stones is commissioned by clinical commissioning groups. Providers are NHS hospital trusts and private hospitals.
Resource impact
We estimate that if these recommendations are implemented, they would have the following impact:
- an increase in medical expulsive therapy for stones less than 10 mm
- an increase in SWL and a reduction in surgical interventions (ureteroscopy, or URS) for people with stones that are less than 10 mm who require a surgical intervention
- overall, cost savings for commissioners and efficiencies for providers.
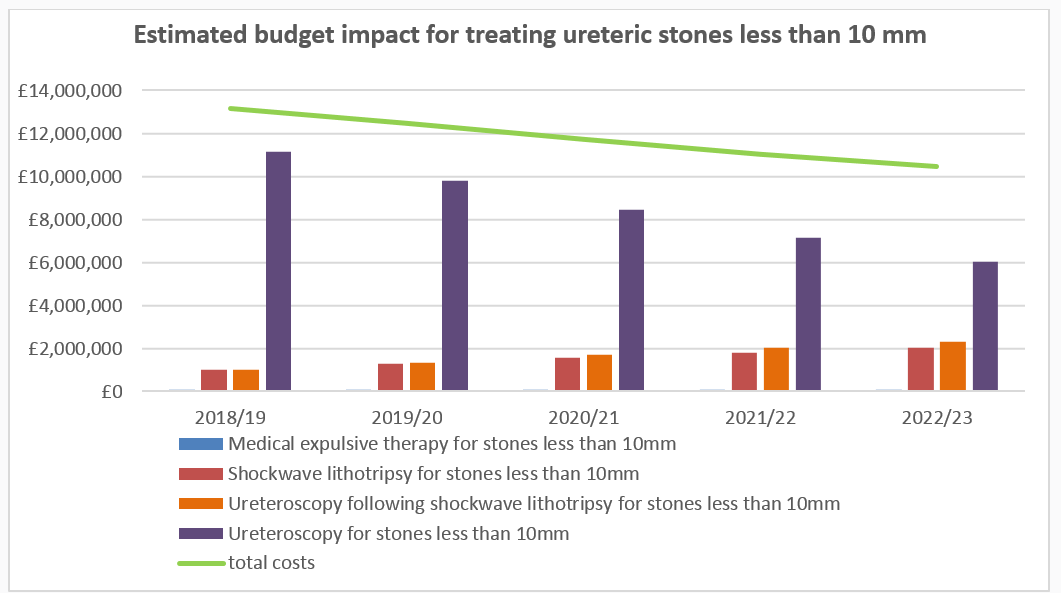
The potential costs and savings to commissioners
The table and graph show the estimated budget impact for treating ureteric stones less than 10 mm over the first 5 years.
| Recommendation |
2018/19 (£000s) |
2019/20 (£000s) |
2020/21 (£000s) |
2021/22 (£000s) |
2022/23 (£000s) |
| Current costs | |||||
| Medical expulsive therapy | 17 | 17 | 17 | 17 | 17 |
| Ureteroscopy | 11,408 | 11,408 | 11,408 | 11,408 | 11,408 |
| Shockwave lithotripsy | 958 | 958 | 958 | 958 | 958 |
| Ureteroscopy following shockwave lithotripsy | 922 | 922 | 922 | 922 | 922 |
| Total costs | 13,305 | 13,305 | 13,305 | 13,305 | 13,305 |
| Future costs | |||||
| Medical expulsive therapy | 20 | 38 | 55 | 73 | 87 |
| Ureteroscopy | 11,140 | 9,801 | 8,461 | 7,122 | 6,050 |
| Shockwave lithotripsy | 1,011 | 1,277 | 1,542 | 1,808 | 2,020 |
| Ureteroscopy following shockwave lithotripsy | 991 | 1,337 | 1,682 | 2,028 | 2,305 |
| Total costs | 13,163 | 12,452 | 11,741 | 11,030 | 10,461 |
| Savings - England | 142 | 853 | 1,564 | 2,275 | 2,844 |
| Savings - per 100,000 population | 0.3 | 1.5 | 2.8 | 4.1 | 5.1 |
- Commissioners should be aware of the following:
- the savings estimated (as shown above) are by undertaking less surgical activity (fewer URS) and increasing SWL
- some lithotripsies are ineffective in removing the stone (clinical view is about 40%), so will require a subsequent ureteroscopy
- if there are additional costs needed to establish networks of mobile or fixed lithotripters, it may take longer for savings to be realised.
- Providers should be aware of the following:
- we estimate that, on average, providers would lose tariff income, due to commissioners paying less (see above)
- there would be redistribution of income between providers from moving from surgery to shockwave therapy, because not all providers have lithotripters. In this area there may also be some additional costs associated with increased patient transport (as people require transport to hospital with lithotripters)
- if providers do not have access to an on-site shockwave lithotripter, they should use local network arrangements to ensure people receive treatment within 48 hours
- these changes are likely to free up acute bed capacity and therefore allow providers to manage acute bed capacity more efficiently.
- Commissioners and providers need to be aware of the recommendations within the Getting It Right First Time (GIRFT) Programme National Speciality Report on urology. The report highlights “The aim of urology networking will not be to concentrate all resources in a single location, but to encourage trusts to work together to balance workload, provide timely and appropriate care (especially emergency care) and ensure patients are treated by teams with greater experience in their condition.”
Support to put the recommendations into practice
- NICE, NHS England and NHS Improvement support improvements in the treatment for renal and ureteric stones and more effective use of NHS resources.
- The Urology GIRFT Programme National Specialty Report on urology highlights the steps to improving treatment of urinary tract stones. See recommendation 9 - Improve the secondary care pathway for patients with urinary stones (page 32).
- The GIRFT programme is currently in discussions with providers to seek to develop urology area networks and identify examples of best practice, which may support implementation of these guidelines.
| The guideline resource and implementation panel |
|
The guideline resource and implementation panel reviews NICE guidelines that have a substantial impact on NHS resources. By ‘substantial’ we mean that:
Panel members are from NICE, NHS England, NHS Improvement, Health Education England and when appropriate Public Health England and Skills for Care. Topic experts are invited for discussions on specific topics. The panel does not comment on or influence the guideline recommendations outside of NICE’s usual consultation processes and timelines. |
This page was last updated: